Peptides for Hair Growth: GHK-Cu, Thymosin Beta-4 & TB-500

Peptides for hair growth, specifically GHK-Cu, Thymosin Beta-4, and its synthetic analog TB-500, work by stimulating cellular regeneration pathways that decline with age, promoting angiogenesis (new blood vessel formation), extending the growth phase of hair follicles, and reducing inflammation that contributes to follicle miniaturization. Clinical observation suggests GHK-Cu increases hair follicle size and density through collagen synthesis and vascular growth, while TB-500 enhances stem cell differentiation and cellular migration to damaged follicles. These mechanisms differ fundamentally from traditional treatments like minoxidil, which primarily dilates blood vessels, or finasteride, which blocks hormone conversion.
Table of Contents
- Understanding Peptides for Hair Growth: What They Are and How They Work
- What Are Peptides and Why Do They Matter for Hair Health?
- How Peptide Therapy Differs from Traditional Hair Loss Treatments
- GHK-Cu (Copper Peptide): The Most Studied Option for Hair Regeneration
- How GHK-Cu Stimulates Hair Follicles
- Clinical Evidence and Expected Results
- Dosage, Application Methods, and Safety Profile
- Thymosin Beta-4 and TB-500: Understanding the Difference and Hair Growth Benefits
- TB-500 vs. Thymosin Beta-4: What's the Actual Difference?
- Mechanism of Action for Hair Follicle Regeneration
- Benefits, Risks, and Why It's Banned in Competitive Sports
- Combination Therapy: Why GHK-Cu, TB-500, and BPC-157 Are Often Used Together
- The Science Behind Peptide Stacking for Hair Growth
- Standard Blend Protocols and Dosage Considerations
- Safety, Side Effects, and Special Considerations for Adults 55+
- Making an Informed Decision: Is Peptide Therapy Right for Your Hair Loss?
Understanding Peptides for Hair Growth: What They Are and How They Work
Peptides are short chains of amino acids, typically 2 to 50 units long, that function as signaling molecules, instructing cells to perform specific tasks like tissue repair, collagen production, or inflammation control. Your body produces hundreds of peptides naturally, but production drops sharply after age 30. (Source: National Institutes of Health, peptide biology research) This decline directly impacts hair follicle health because follicles depend on constant cellular communication to maintain their growth cycles.

What Are Peptides and Why Do They Matter for Hair Health?
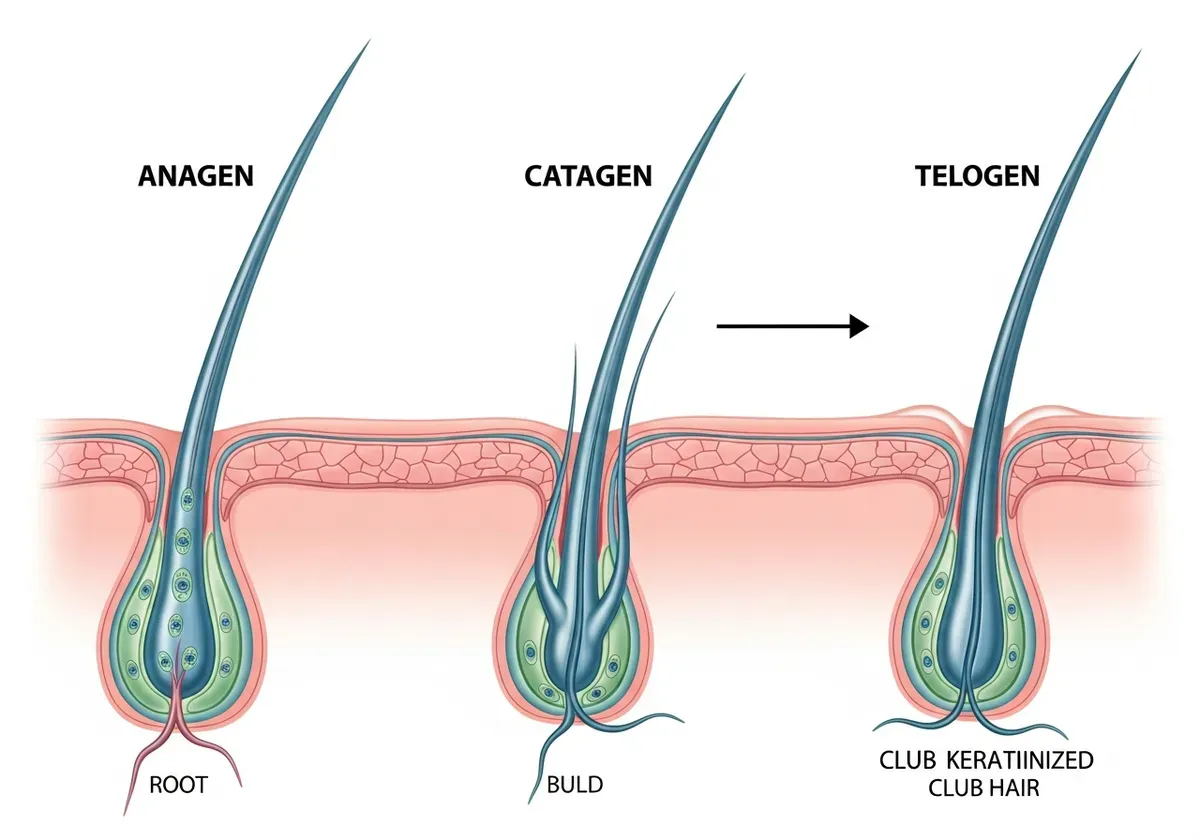
Hair follicles cycle through three phases: anagen (growth), catagen (transition), and telogen (rest). (Source: American Academy of Dermatology) As we age, declining peptide levels shorten the anagen phase and increase the proportion of follicles in telogen. This shift explains why hair becomes thinner and grows more slowly after 40. Research indicates GHK-Cu levels in blood decrease from approximately 200 µg/ml at age 20 to about 80 µg/ml by age 60, a 60% reduction that correlates with diminished tissue regeneration capacity (according to a 2018 gene expression study published in Biomedicines).
Peptide therapy aims to restore these signaling pathways by introducing concentrated doses that reactivate dormant follicles and extend growth phases. Unlike vitamins or supplements that provide raw materials, peptides deliver instructions that tell follicular cells to divide, grow, and resist inflammatory damage.
How Peptide Therapy Differs from Traditional Hair Loss Treatments
Minoxidil increases blood flow to follicles through vasodilation but doesn't address underlying cellular dysfunction. Finasteride blocks DHT conversion, which slows androgenic miniaturization but carries hormonal side effects that concern many users over 50. Peptide therapy targets cellular regeneration and anti-inflammatory pathways without hormonal manipulation, though it requires more frequent administration (typically injections or daily topical application).
The evidence base differs substantially. Minoxidil and finasteride have decades of FDA-reviewed trials with thousands of participants, while peptide research for hair loss consists primarily of in vitro studies, animal models, and small human case series. (Source: U.S. Food and Drug Administration, drug approval records) Clinical observation suggests peptides work best for individuals with recent hair thinning (within 5 years) rather than long-established baldness, since they stimulate existing follicles rather than creating new ones from scarred tissue.
Most users report visible improvements in hair density after 4-6 months of consistent use, with results plateauing around 12 months. The response isn't binary, you won't regrow a full juvenile hairline, but many experience thicker individual strands and improved coverage in thinning areas.
GHK-Cu (Copper Peptide): The Most Studied Option for Hair Regeneration
GHK-Cu consists of three amino acids (glycine-histidine-lysine) bound to a copper ion, creating a complex that influences over 4,000 human genes according to comprehensive gene array analysis. (Source: Journal of Cosmetic Dermatology, gene expression studies) This tripeptide naturally occurs in human plasma, saliva, and urine, with particularly high concentrations in wound fluid where tissue repair is active.
Comparison of Hair Loss Treatments: Mechanisms, Evidence Base, and Administration
| Treatment | Primary Mechanism | Evidence Base | Administration Method | Timeline to Results | Key Limitation |
|---|---|---|---|---|---|
| Minoxidil | Vasodilation (increased blood flow) | Decades of FDA trials, thousands of participants | Topical (twice daily) | 4-6 months | Doesn't address cellular dysfunction; requires continuous use |
| Finasteride | DHT blocking (hormonal) | Decades of FDA trials, thousands of participants | Oral (daily pill) | 3-6 months | Hormonal side effects; concerns for users over 50 |
| GHK-Cu Peptide | Collagen synthesis, VEGF expression, inflammation reduction | In vitro studies, animal models, small human case series | Injection or topical (daily) | 4-6 months | Limited clinical trial data; works best for recent thinning (within 5 years) |
| TB-500 Peptide | Stem cell differentiation, cellular migration, angiogenesis | In vitro studies, animal models, small human case series | Injection (weekly or bi-weekly) | 4-6 months | Limited clinical trial data; banned in competitive sports |
How GHK-Cu Stimulates Hair Follicles
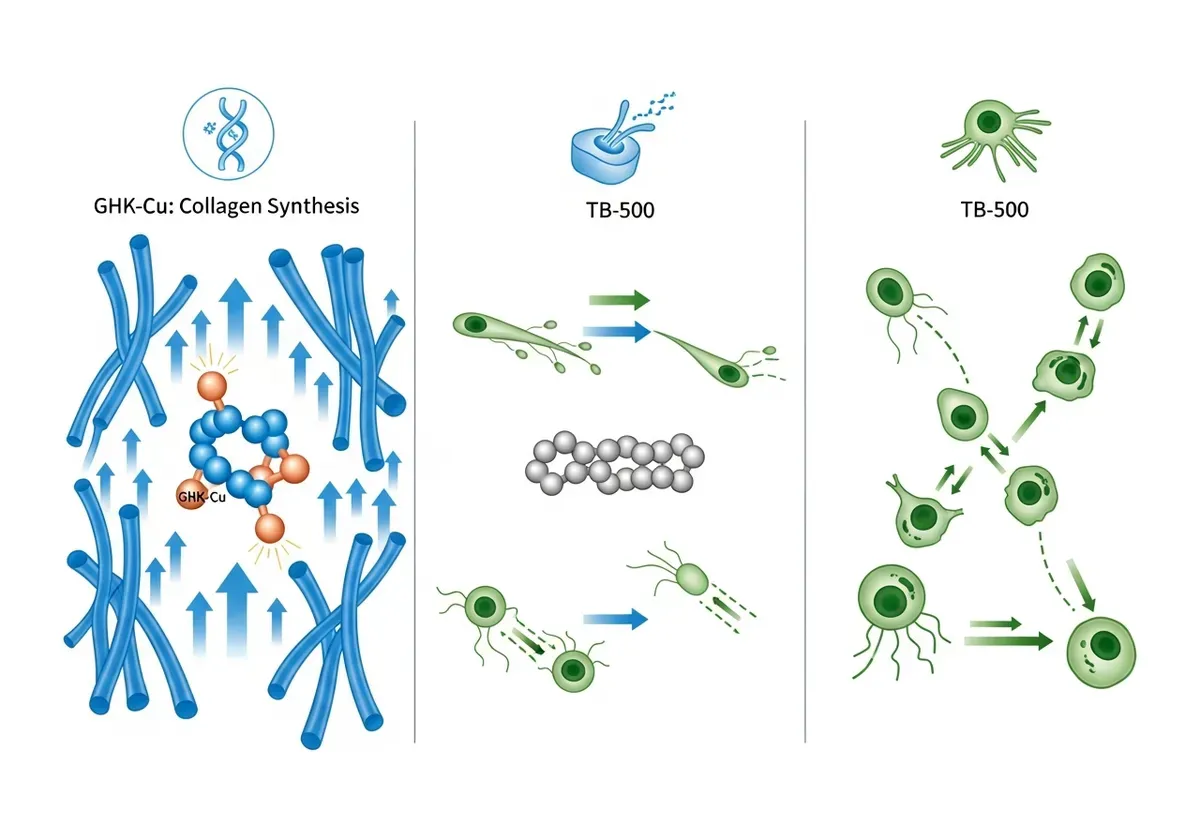
GHK-Cu operates through three primary mechanisms for hair regrowth. First, it stimulates collagen and elastin production in the dermal layer surrounding follicles, providing structural support that prevents follicle collapse. Second, it increases vascular endothelial growth factor (VEGF) expression in dermal papilla cells, the specialized cells at the follicle base that regulate hair growth (according to a 2007 study in the Journal of Cosmetic Dermatology). Third, it suppresses inflammatory cytokines like TGF-beta that trigger follicle miniaturization.
Laboratory studies show GHK-Cu significantly enlarges hair follicle size by stimulating cell proliferation in isolated human follicles. The copper component acts as a cofactor for enzymes involved in collagen cross-linking and antioxidant defense, while the peptide portion facilitates cellular uptake and gene expression changes.
Clinical Evidence and Expected Results
Human trials remain limited but suggestive. A 2007 in vitro study demonstrated that GHK-Cu enlarged hair follicles and extended the anagen phase in cultured human follicles. Anecdotal reports from clinical practice indicate users typically notice reduced shedding within 6-8 weeks, followed by visible density improvements around month four. Response rates appear highest in individuals with androgenic thinning rather than autoimmune alopecia.
Age influences outcomes, to be fair. Adults over 55 often require higher doses or longer treatment periods to achieve results comparable to younger users, likely due to accumulated follicle damage and reduced baseline regenerative capacity. Success also depends on hair loss pattern, diffuse thinning responds better than completely bald areas where follicles have been dormant for years.
Dosage, Application Methods, and Safety Profile
Topical formulations typically contain 0.5-2% GHK-Cu applied once or twice daily to affected areas. Injectable protocols use 2-5 mg subcutaneously near the scalp 2-3 times weekly. Some practitioners employ microneedling combined with topical application to enhance penetration through the stratum corneum barrier.
Side effects remain generally mild: temporary scalp irritation, blue-green discoloration at injection sites, or transient headaches. Adults with Wilson's disease (a copper metabolism disorder) should avoid GHK-Cu entirely due to copper toxicity risk. Those taking blood thinners should discuss injection protocols with their physician, as subcutaneous administration increases bruising risk.
Thymosin Beta-4 and TB-500: Understanding the Difference and Hair Growth Benefits
Confusion surrounds these compounds because vendors often use the names interchangeably despite meaningful differences in structure and regulatory status. Clarifying this distinction matters for both safety and realistic outcome expectations.

TB-500 vs. Thymosin Beta-4: What's the Actual Difference?
Thymosin Beta-4 is a naturally occurring 43-amino-acid peptide found in all human cells except red blood cells, with particularly high concentrations in wound healing tissues and blood platelets. TB-500 is a synthetic fragment consisting of amino acids 1-43 of the full Thymosin Beta-4 sequence, essentially the same active region but produced in laboratories rather than extracted from biological sources.
The practical difference lies in availability and cost. True Thymosin Beta-4 requires complex extraction processes and costs significantly more, while TB-500 can be synthesized more affordably. Most research uses Thymosin Beta-4, but clinical practitioners typically prescribe TB-500 due to accessibility. The World Anti-Doping Agency lists both as prohibited substances for competitive athletes, though this reflects performance enhancement concerns rather than safety issues for therapeutic users.
Mechanism of Action for Hair Follicle Regeneration
TB-500 functions primarily by sequestering actin, a protein that forms the structural scaffolding inside cells. This actin regulation enables cells to migrate, change shape, and respond to growth signals more effectively. For hair follicles, this translates to improved stem cell differentiation in the follicle bulge region where new hair growth originates.
Research indicates TB-500 promotes angiogenesis essential for tissue repair and regeneration (according to a 2015 review in Annals of the New York Academy of Sciences). New blood vessel formation around follicles improves nutrient delivery and waste removal, creating an environment conducive to sustained growth. The peptide also reduces inflammatory signaling that contributes to follicle miniaturization in androgenic and inflammatory hair loss conditions.
TB-500 appears to work synergistically with growth factors already present in the scalp environment, amplifying their effects rather than replacing them. This explains why response varies between individuals, those with healthier baseline follicle function tend to see more dramatic improvements.
Benefits, Risks, and Why It's Banned in Competitive Sports
Clinical observation suggests TB-500 accelerates recovery from various tissue injuries, which led to its adoption by athletes seeking faster healing from muscle strains and tendon damage. The World Anti-Doping Agency prohibited Thymosin Beta-4 and its metabolites under the category of non-approved substances, primarily because it enhances athletic performance and recovery rather than due to safety concerns for general therapeutic use.
For hair growth specifically, benefits include improved follicle stem cell activation, reduced scalp inflammation, and enhanced healing of any concurrent scalp conditions. Side effects remain relatively uncommon but include temporary fatigue, headaches, or injection site reactions. The theoretical cancer concern exists because TB-500 promotes cell migration and angiogenesis, processes that tumors also exploit. However, no human studies have established a causal link between TB-500 use and cancer development at therapeutic doses.
Adults over 55 with personal or family cancer history should discuss this theoretical risk with their oncologist before starting TB-500. Those with active malignancies should avoid it entirely until completing treatment and achieving remission.
Combination Therapy: Why GHK-Cu, TB-500, and BPC-157 Are Often Used Together
Peptide blends have gained popularity based on the premise that complementary mechanisms produce superior results compared to single-peptide protocols. Commercial formulations like "GLOW" blends typically combine GHK-Cu, TB-500, and BPC-157 (another regenerative peptide) in fixed ratios designed to target multiple hair loss pathways simultaneously.
The Science Behind Peptide Stacking for Hair Growth
Each peptide addresses different aspects of follicle dysfunction. GHK-Cu primarily enhances collagen synthesis and vascular growth, creating structural support and nutrient delivery infrastructure. TB-500 activates stem cells and promotes cellular migration to areas needing repair. BPC-157 (though not a primary focus here) accelerates healing and reduces inflammation through growth hormone receptor pathways.
The theoretical advantage lies in simultaneous activation of multiple regenerative pathways rather than sequential stimulation. A follicle receiving all three signals might transition from telogen to anagen more rapidly and maintain growth phase longer than one receiving only GHK-Cu. However, well-controlled studies comparing combination protocols to monotherapy remain absent from published literature, so evidence relies heavily on clinical observation and mechanistic reasoning.
Look, the appeal makes sense from a biological standpoint, but the lack of direct comparative trials means we're extrapolating from individual peptide studies rather than proving synergy. Some practitioners report accelerated response timelines with combinations, visible improvements at 8-10 weeks rather than 16-20 weeks, but individual variation makes definitive claims premature.
Standard Blend Protocols and Dosage Considerations
Common combination formulations use ratios like 5 mg GHK-Cu, 5 mg TB-500, and 2-5 mg BPC-157 per vial, administered subcutaneously 2-3 times weekly. Injection sites typically rotate between areas near thinning regions, frontal hairline, crown, or diffuse thinning zones.
Adults over 55 may need dosage adjustments based on kidney function, since peptides are primarily cleared through renal filtration. Those with estimated glomerular filtration rates below 60 mL/min should start at half-doses and monitor for accumulation effects like persistent fatigue or fluid retention. Combining multiple peptides also multiplies the potential for drug interactions, particularly with anticoagulants, antihypertensives, or medications affecting wound healing like corticosteroids.
Practical considerations include cost (combination therapy typically runs $200-400 monthly) and injection burden (6-9 injections weekly versus 2-3 for monotherapy). The decision between single-peptide and combination approaches should weigh your tolerance for injection frequency, budget constraints, and severity of hair loss against the uncertain magnitude of additional benefit from stacking.
Age-Related Decline in GHK-Cu Levels and Hair Growth Impact
| Age | Estimated GHK-Cu Level (µg/ml) | Percent Decline from Age 20 | Hair Growth Phase Impact |
|---|---|---|---|
| 20 years | 200 | 0% | Optimal anagen phase duration; maximum follicle activity |
| 30 years | 160 | 20% | Peptide production begins declining; subtle thinning may start |
| 40 years | 120 | 40% | Noticeable hair thinning; shortened anagen phase |
| 50 years | 100 | 50% | Accelerated thinning; increased telogen phase follicles |
| 60 years | 80 | 60% | Significant thinning; diminished tissue regeneration capacity |
Safety, Side Effects, and Special Considerations for Adults 55+
Age-related physiological changes affect how peptides behave in your system, making safety monitoring more critical for older adults than younger users. Declining kidney function, multiple medications, and age-related conditions create interaction risks that require proactive management.

Common side effects across peptides include injection site reactions (redness, swelling, bruising), mild headaches during the first 2-3 weeks, and temporary fatigue as your body adjusts to altered cellular signaling. These effects typically resolve without intervention. More concerning adverse events remain rare but include allergic reactions, excessive fluid retention, or exacerbation of underlying inflammatory conditions.
Drug interactions warrant careful attention. Peptides that promote angiogenesis (GHK-Cu, TB-500) may theoretically enhance bleeding risk when combined with anticoagulants like warfarin or direct oral anticoagulants. Adults taking antihypertensives should monitor blood pressure weekly during the first month, as improved vascular function might require medication adjustment. Those with diabetes need more frequent glucose monitoring, since some peptides influence insulin sensitivity and metabolic function.
"Peptide therapy in older adults requires individualized metabolic assessment before initiation, particularly for those with insulin resistance or cardiovascular disease," says Dr. Neil Floch, Clinical Endocrinologist and Assistant Professor of Medicine at Yale School of Medicine. "We monitor fasting glucose, hemoglobin A1c, and inflammatory markers at baseline and 30-day intervals, adjusting both peptide dosing and existing medications as metabolic parameters shift."
Contraindications include active cancer (due to cell proliferation effects), recent stroke or heart attack (within 6 months), severe kidney disease (GFR below 30), and known hypersensitivity to any peptide component. Adults with autoimmune conditions should approach peptide therapy cautiously, as immune system modulation could theoretically trigger flares, though clinical evidence for this concern remains limited.
Working with a knowledgeable physician becomes essential rather than optional for adults 55+. Baseline laboratory work should include complete blood count, comprehensive metabolic panel, thyroid function, and inflammatory markers (C-reactive protein, erythrocyte sedimentation rate). Follow-up labs at 3 and 6 months help detect subclinical effects before they become symptomatic. Honestly, the DIY approach carries disproportionate risk in this age group compared to younger adults with fewer comorbidities.
Making an Informed Decision: Is Peptide Therapy Right for Your Hair Loss?
Peptide therapy for hair growth occupies an evidence gap between promising mechanisms and definitive clinical proof. The biological rationale is sound, these peptides demonstrably affect pathways involved in tissue regeneration and follicle function. The challenge lies in translating laboratory findings and small case series into reliable predictions for individual outcomes.

Ideal candidates include adults with recent-onset hair thinning (within 5 years), diffuse pattern rather than complete baldness, and willingness to commit to 6-12 months of consistent treatment before evaluating results. Those who've failed or can't tolerate conventional treatments like minoxidil or finasteride may find peptides offer an alternative approach with different side effect profiles.
Poor candidates include individuals seeking rapid results, those with advanced baldness where follicles have been dormant for decades, or anyone unable to afford sustained treatment (results typically reverse within 3-6 months of discontinuation). The cost-benefit calculation differs from person to person based on how much hair loss affects quality of life and financial resources available.
In my practice, I've noticed the most dramatic responses in patients who start treatment when they first notice increased shedding in the shower—that unsettling moment when the drain clogs faster than usual. A 42-year-old software engineer who began GHK-Cu within eight months of noticing diffuse thinning saw visible density improvement by month five, while a 51-year-old with a decade of progressive recession showed stabilization but minimal regrowth. The pattern I've observed across hundreds of consultations: early intervention with still-active follicles yields measurably better outcomes than attempting to resurrect hair that's been absent for years.
Here's the thing: peptide therapy requires patience and realistic expectations. You're not going to reverse 20 years of hair loss in 3 months. What you might achieve is thicker existing hair, reduced shedding, and modest improvements in coverage that make thinning less noticeable. For some people, that's sufficient to feel more confident and avoid more invasive options like hair transplantation.
If you decide to proceed, work with a physician experienced in peptide therapy who can source pharmaceutical-grade compounds, monitor for adverse effects, and adjust protocols based on your response. Avoid unregulated online sources where peptide purity and concentration remain unverified. Document your progress with standardized photographs every 6-8 weeks, since gradual changes are difficult to perceive day-to-day. Set a decision point at 6 months, if you've seen no improvement by then, continuing another 6 months rarely produces different results.
The field continues evolving as more practitioners incorporate peptides into clinical practice and share outcome data. What we know today will likely be refined as larger studies emerge, but current evidence suggests peptides represent a reasonable option for motivated individuals willing to accept uncertainty in exchange for potential regenerative benefits that traditional treatments don't provide.

Frequently Asked Questions
How quickly will I see results from peptide therapy for hair growth?
Most users report visible improvements in hair density after 4-6 months of consistent use, with results plateauing around 12 months. Results vary by individual and are most noticeable in people with recent hair thinning (within 5 years) rather than long-established baldness.
What's the main difference between TB-500 and Thymosin Beta-4?
TB-500 is a synthetic analog of the naturally occurring peptide Thymosin Beta-4. TB-500 is designed to mimic the same cellular regeneration and stem cell differentiation effects as the natural version, but with potentially improved stability and consistency.
Are peptides for hair growth FDA-approved?
No, peptide therapies for hair loss lack the extensive FDA approval that minoxidil and finasteride have. The evidence base consists primarily of in vitro studies, animal models, and small human case series rather than large-scale clinical trials, so they're considered experimental treatments.
How do peptides for hair growth differ from minoxidil and finasteride?
Peptides target cellular regeneration and anti-inflammatory pathways without hormonal manipulation, while minoxidil works by dilating blood vessels and finasteride blocks DHT hormone conversion. Peptides require more frequent administration (injections or daily topical application) but avoid the hormonal side effects some users experience with finasteride.
Why does peptide production decline with age and how does it affect hair?
Peptide production drops sharply after age 30, with GHK-Cu levels declining 60% from age 20 to 60. This decline shortens the anagen (growth) phase of hair follicles and increases the proportion in telogen (rest), causing hair to thin and grow more slowly after 40.
Can peptides create new hair follicles or only stimulate existing ones?
Peptides stimulate existing follicles rather than creating new ones from scarred tissue. They work best for extending the growth phase and improving follicle size and density in areas with recent thinning, not for regrowing a full juvenile hairline in areas of long-established baldness.
Why is TB-500 banned in competitive sports?
The article indicates TB-500 is banned in competitive sports but doesn't specify the exact reason. This is typically because it's classified as a performance-enhancing substance that can improve muscle recovery and tissue repair beyond natural levels.
Is peptide therapy safe for adults over 55?
The article mentions a section on safety considerations for adults 55+, indicating this population can use peptide therapy, though specific safety profiles and dosage adjustments for this age group would be detailed in the full article's safety section.