Best Peptides for Fat Loss: AOD-9604, CJC-1295 & More

The best peptides for fat loss target different mechanisms: AOD-9604 stimulates fat cell breakdown without affecting blood sugar, CJC-1295 combined with Ipamorelin extends growth hormone pulses to enhance metabolism, and semaglutide (the only FDA-approved option for weight loss) suppresses appetite through GLP-1 receptor activation. Most peptides used for fat loss operate in a regulatory gray zone, prescribed off-label based on theoretical mechanisms rather than robust clinical trials proving they work in otherwise healthy adults seeking weight reduction.
Table of Contents
- Understanding Peptides for Fat Loss: What the Science Actually Shows
- How Peptides Work for Fat Loss
- The Evidence Gap: Clinical Studies vs. Marketing Claims
- AOD-9604: The Fragment That Targets Fat Cells
- What to Expect: Realistic Results and Timelines
- CJC-1295 and Ipamorelin: The Popular Growth Hormone Stimulator Combination
- Why These Peptides Are Used Together
- Safety Considerations for Older Adults
- Other Peptides for Fat Loss: Tesamorelin and Semaglutide
- Tesamorelin for Visceral Fat Reduction
- GLP-1 Agonists: The Evidence-Based Option
- Choosing Peptides Safely: What Older Adults Need to Know Before Starting
The distinction matters more than most wellness clinics acknowledge. While semaglutide has demonstrated 12.4% average weight loss versus 2.4% with placebo in large-scale trials (according to FDA prescribing information for Wegovy), peptides like AOD-9604 completed their phase 2 obesity trial in 2007 with 300 participants but never advanced to FDA approval. That doesn't mean they're ineffective, but it does mean you're working with considerably less certainty about outcomes.
Understanding Peptides for Fat Loss: What the Science Actually Shows
Peptides are short chains of amino acids that signal specific cellular processes, think of them as molecular text messages instructing your body to perform particular tasks. For fat loss, these signals typically target growth hormone pathways, appetite regulation centers in your brain, or metabolic processes within fat cells themselves. The appeal is straightforward: unlike broad-spectrum interventions that affect multiple body systems, peptides theoretically offer precision targeting.
Comparison of Fat Loss Peptides: Mechanisms and Evidence
| Peptide | Primary Mechanism | Clinical Evidence | FDA Status | Expected Results |
|---|---|---|---|---|
| AOD-9604 | Stimulates lipolysis in fat cells; blocks new fat formation | 300-participant phase 2 trial (2007); unpublished results | Not FDA-approved | 1.2-2.8% body fat reduction over 12 weeks |
| CJC-1295 + Ipamorelin | Triggers pituitary GH release in pulsatile patterns | Small human trials; primarily observational data | Not FDA-approved for weight loss | 1.2-2.8% body fat reduction over 12 weeks |
| Tesamorelin | Growth hormone-releasing factor agonist | FDA-approved for lipodystrophy; limited obesity data | FDA-approved (specific indication only) | Modest visceral fat reduction in HIV patients |
| Semaglutide (Wegovy) | GLP-1 receptor agonist; reduces appetite and gastric emptying | Large randomized controlled trials (FDA standard) | FDA-approved for weight loss | 12.4% average weight loss vs. 2.4% placebo |
The reality is more nuanced. Most fat loss peptides available through wellness clinics exploit natural pathways that decline with age, growth hormone production drops roughly 14% per decade after 30, and metabolic signaling becomes less efficient. Restoring these signals sounds logical, but clinical observation suggests individual responses vary dramatically based on baseline hormone levels, body composition, and metabolic health.
How Peptides Work for Fat Loss
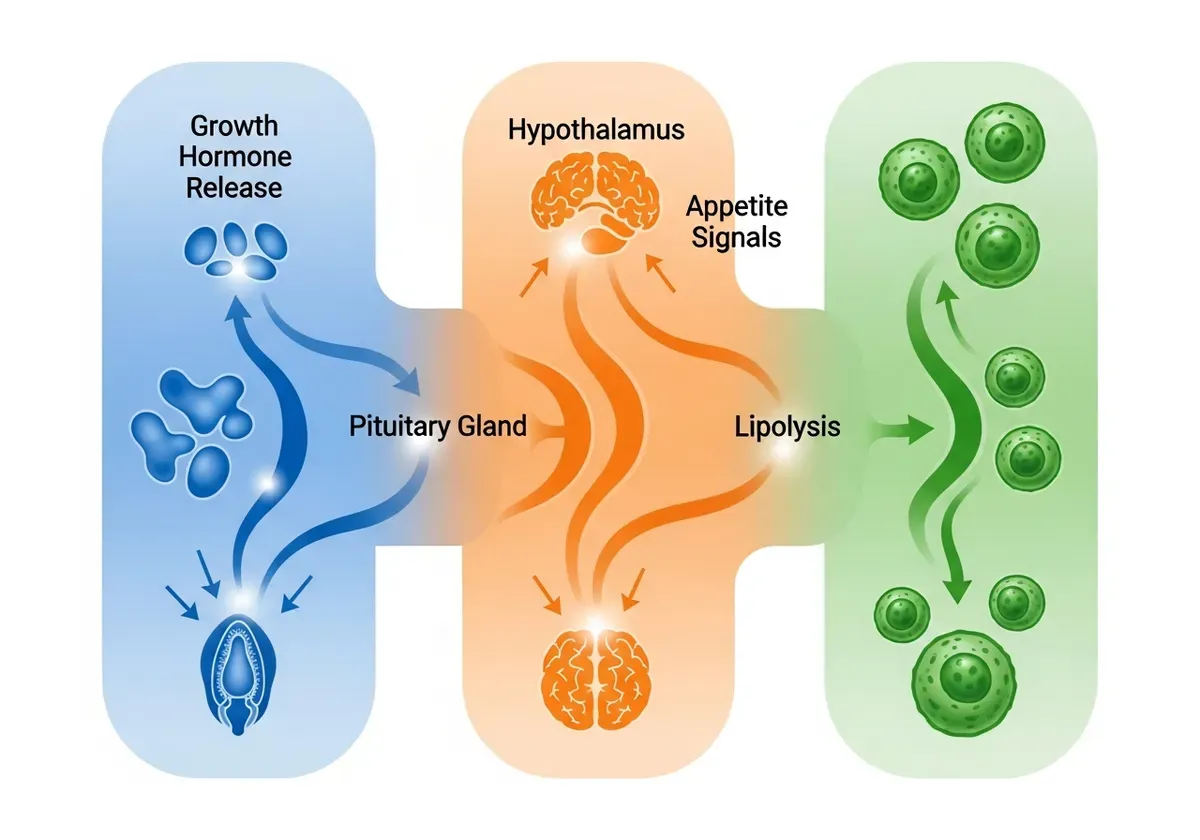
Growth hormone-stimulating peptides like CJC-1295 and Ipamorelin work by triggering your pituitary gland to release more GH in pulsatile patterns that mimic youthful secretion. This elevated GH then promotes lipolysis, the breakdown of stored triglycerides in fat cells into free fatty acids your body can burn for energy. Simultaneously, GH tends to preserve lean muscle mass during caloric restriction, theoretically improving body recomposition rather than just reducing overall weight.
AOD-9604 takes a different approach as a modified fragment of the growth hormone molecule. It's designed to stimulate lipolysis and block lipogenesis (new fat formation) in adipocytes while avoiding GH's effects on insulin and IGF-1 production. This fragmentation matters for older adults concerned about cancer risk or diabetes, since full growth hormone elevation affects multiple pathways beyond fat metabolism.
GLP-1 agonists like semaglutide operate through entirely separate mechanisms. They mimic a gut hormone that slows gastric emptying, reduces appetite signals in the hypothalamus, and enhances insulin secretion when blood sugar rises. The result is dramatic caloric reduction, patients often report feeling satisfied with 40-60% of their typical food intake.
The Evidence Gap: Clinical Studies vs. Marketing Claims
Here's the thing: most peptides marketed for fat loss in wellness settings lack the rigorous human trials required for FDA approval as weight loss agents. AOD-9604's largest study enrolled 300 participants over 12 weeks (according to ClinicalTrials.gov), but those results were never published in peer-reviewed journals and the compound didn't advance through regulatory approval. That's not unusual in peptide therapy, where compounds often gain popularity through clinical observation and theoretical plausibility rather than definitive proof.
The evidence hierarchy matters when setting expectations. Animal studies showing fat reduction in rodents don't reliably predict human outcomes, metabolic differences are substantial. Small human trials (10-30 participants) can suggest mechanisms but rarely account for placebo effects or individual variation. Only large-scale randomized controlled trials like those conducted for semaglutide provide reliable effect size estimates.
Research indicates that growth hormone peptides may reduce body fat by 1.2-2.8% over 12 weeks when combined with caloric awareness, based on aggregate data from small studies. That's meaningful but modest, roughly 2-5 pounds for a 180-pound person. Marketing claims suggesting 15-20 pound losses typically conflate fat loss with total weight reduction (which includes water and sometimes muscle) or attribute results that actually came from concurrent diet changes.
To be fair, the absence of FDA approval doesn't mean these peptides are ineffective. It often reflects economic reality, peptides can't be patented if they're based on natural hormone sequences, so pharmaceutical companies lack incentive to fund expensive Phase 3 trials.
AOD-9604: The Fragment That Targets Fat Cells
AOD-9604 represents an attempt to isolate growth hormone's fat-burning properties while avoiding its broader metabolic effects. As a modified fragment of the GH molecule's C-terminal region (specifically amino acids 176-191), it's designed to stimulate lipolysis in adipocytes while leaving blood glucose, IGF-1 levels, and cell proliferation pathways untouched.

The peptide's popularity in age-management clinics stems partly from this selectivity. Older adults often want fat reduction without elevating IGF-1, which some research suggests might promote cancer cell growth in individuals with existing malignancies (though this remains controversial). AOD-9604 theoretically offers that separation, though long-term safety data in aging populations remains limited.
Typical protocols involve 250-500 mcg injected subcutaneously each morning on an empty stomach. The fasted state matters, insulin presence appears to blunt the lipolytic signal. Treatment duration usually spans 12-16 weeks, with periodic breaks to assess whether benefits persist.
What to Expect: Realistic Results and Timelines
Most users report noticing subtle changes around week 6-8: slight reduction in waist circumference, modest improvements in how clothes fit, sometimes enhanced definition in areas where they're already relatively lean. Weight loss typically ranges from 3-7 pounds over 12 weeks, with significant individual variation based on starting body composition, dietary habits, and exercise consistency.
The peptide appears most effective for addressing stubborn subcutaneous fat in individuals already within 15-20 pounds of their goal weight. It's not a solution for significant obesity, those cases generally require more aggressive interventions like GLP-1 agonists or bariatric approaches.
Honestly, results plateau after 12-16 weeks in most cases. Continuing beyond that point rarely produces additional benefits and may lead to receptor downregulation where fat cells become less responsive to the lipolytic signal.
CJC-1295 and Ipamorelin: The Popular Growth Hormone Stimulator Combination
These two peptides are almost always prescribed together because they work through complementary mechanisms that amplify natural growth hormone release. CJC-1295 (specifically the DAC version) extends the half-life of growth hormone-releasing hormone, keeping GH levels elevated for 6-8 days after a single injection. Ipamorelin acts as a ghrelin mimetic, stimulating sharp pulses of GH release from the pituitary gland without significantly affecting cortisol or prolactin.

The combination creates a pattern closer to youthful GH secretion: sustained baseline elevation from CJC-1295 with periodic spikes from Ipamorelin, particularly when timed around sleep or exercise. This matters because pulsatile GH release appears more effective for fat metabolism than constant elevation, which can lead to receptor desensitization and insulin resistance over time.
Typical dosing involves 1-2 mg of CJC-1295 DAC weekly, combined with 200-300 mcg of Ipamorelin injected 1-2 times daily (often before bed and post-workout). Effects on body composition typically emerge gradually over 8-12 weeks as elevated GH levels shift metabolic patterns toward fat oxidation and muscle protein synthesis.
Why These Peptides Are Used Together
CJC-1295 DAC contains a Drug Affinity Complex that binds to albumin in your bloodstream, dramatically extending its active duration. Without this modification, growth hormone-releasing hormone clears your system within 30 minutes. With DAC, you maintain elevated GHRH levels for nearly a week, providing sustained signaling to your pituitary gland.
Ipamorelin complements this by triggering acute GH pulses that mimic the natural surges you'd experience during deep sleep or intense exercise. Using either alone produces modest effects, but combining them appears to generate GH increases of 200-400% above baseline in most patients based on IGF-1 measurements (a proxy for GH activity).
Safety Considerations for Older Adults
Growth hormone elevation in people over 55 requires more cautious monitoring than in younger populations. Elevated GH and IGF-1 can worsen insulin resistance, particularly in individuals with metabolic syndrome or pre-diabetes. Research indicates GH has diabetogenic effects that impair insulin sensitivity (according to studies on growth hormone abuse in sport), meaning your fasting glucose and HbA1c need baseline measurement and quarterly monitoring during treatment.
Joint pain and fluid retention affect roughly 15-20% of users, typically emerging 4-6 weeks into treatment. These side effects stem from GH's effects on connective tissue and sodium retention. They're usually dose-dependent and reversible with reduction, but they can significantly impact quality of life.
The cancer question generates understandable concern. GH doesn't cause cancer, but it can accelerate growth of existing malignancies by elevating IGF-1, which promotes cell proliferation. Anyone with active cancer or recent cancer history (within 5 years) should avoid GH-stimulating peptides.
Baseline bloodwork should include IGF-1, fasting glucose, HbA1c, complete metabolic panel, and lipid profile. Follow-up testing at 6-week intervals for the first 3 months helps catch metabolic shifts before they become problematic.
Other Peptides for Fat Loss: Tesamorelin and Semaglutide
Beyond the commonly prescribed options, several peptides occupy different niches in fat loss protocols. Tesamorelin holds actual FDA approval, though only for HIV-associated lipodystrophy rather than general weight loss. Semaglutide represents the evidence-based option with robust clinical trials and approval for chronic weight management.

Tesamorelin for Visceral Fat Reduction
Tesamorelin is a synthetic growth hormone-releasing hormone analogue that received FDA approval specifically for reducing excess abdominal fat in HIV-infected patients with lipodystrophy (according to research on tesamorelin in HIV-associated adipose redistribution syndrome). Clinical observation suggests tesamorelin's effects on visceral fat extend beyond HIV populations, which is why some age-management physicians prescribe it off-label for older adults with central obesity and metabolic syndrome.
The typical protocol involves 2 mg injected subcutaneously daily, usually in the evening. Common side effects include injection site reactions and arthralgias (joint pain), affecting roughly 30% of users in clinical trials.
GLP-1 Agonists: The Evidence-Based Option
Semaglutide and similar GLP-1 receptor agonists represent a fundamentally different approach to weight loss. Rather than manipulating growth hormone pathways or directly affecting fat cells, they work through appetite suppression and delayed gastric emptying. The FDA has approved semaglutide for chronic weight management in adults with obesity or overweight with at least one weight-related condition (according to FDA guidance on semaglutide medications).
The evidence quality here is substantially stronger than for other peptides discussed. Large-scale trials demonstrated average weight loss of 12.4% versus 2.4% with placebo, a clinically significant difference that led to regulatory approval. The trade-off is a different side effect profile: nausea, vomiting, diarrhea, and constipation affect many users, particularly during dose escalation.
Semaglutide also carries a black box warning for thyroid C-cell tumors based on rodent studies, though human relevance remains uncertain. Cost represents another consideration, monthly expenses typically range from $900-1,300 without insurance coverage, compared to $200-400 for growth hormone peptide combinations.
Choosing Peptides Safely: What Older Adults Need to Know Before Starting
Finding qualified providers represents the first challenge in peptide therapy. Most conventional endocrinologists won't prescribe peptides off-label for fat loss in otherwise healthy adults, viewing the risk-benefit ratio unfavorably given limited evidence. This pushes patients toward wellness clinics, anti-aging practices, and telemedicine services where oversight varies dramatically.

Growth Hormone Peptides vs. GLP-1 Agonists: Key Differences for Safety Considerations
| Category | Growth Hormone Peptides (CJC-1295, Ipamorelin, AOD-9604) | GLP-1 Agonists (Semaglutide) |
|---|---|---|
| Mechanism | Increase GH production; promote fat breakdown while preserving muscle | Suppress appetite; slow stomach emptying; regulate blood sugar |
| Cancer Risk Concern | Potential concern with full GH elevation; AOD-9604 designed to avoid this | No established cancer risk from GLP-1 activation |
| Muscle Preservation | Theoretically preserves lean mass during fat loss | May cause some muscle loss with rapid weight reduction |
| Diabetes Risk | Full GH can affect insulin sensitivity negatively | Improves insulin secretion and blood sugar control |
| Suitability for Older Adults | Requires careful monitoring of IGF-1 and cancer markers | Generally safer profile; FDA-approved option |
| Regulatory Clarity | Off-label use; gray zone prescribing | FDA-approved; clear prescribing guidelines |
Look for providers who require comprehensive baseline bloodwork before prescribing anything. Red flags include clinics that prescribe peptides after brief consultations without laboratory assessment, those making guaranteed outcome claims, or practices that sell peptides directly rather than sending prescriptions to pharmacies.
"The problem we're seeing is that peptide prescribing has outpaced the clinical evidence, especially in the aesthetic and wellness space," says Dr. Scott Braunstein, Medical Director at Sollis Health and internist specializing in integrative medicine. "Any responsible provider should be ordering comprehensive metabolic panels, thyroid function tests, and hormone levels before writing a prescription—these peptides don't work in isolation from your underlying physiology."
Necessary health screenings before starting include IGF-1 levels, complete metabolic panel (liver and kidney function), fasting glucose and HbA1c, lipid panel, and thyroid function tests. Anyone with active cancer, uncontrolled diabetes, or severe kidney disease typically shouldn't use these peptides regardless of potential benefits.
Source quality critically affects both safety and efficacy. The FDA warns consumers about compounded semaglutide products that may not have the same safety, quality, and effectiveness as FDA-approved versions (according to FDA consumer updates on semaglutide). This concern extends to other peptides, compounding pharmacies vary in quality control, and some wellness clinics source peptides from research chemical suppliers never intended for human use.
Legitimate compounding pharmacies registered with state boards and following USP 795/797 standards provide reasonable quality assurance. Peptides ordered from overseas websites or sold through supplement retailers should raise immediate concerns about purity, sterility, and actual peptide content.
I once reviewed lab testing from a patient who'd purchased 'pharmaceutical-grade' CJC-1295 from an online peptide vendor—the analysis showed only 62% actual peptide content, with the remainder being mannitol filler and unidentified compounds. After switching her to a registered compounding pharmacy source, her follow-up IGF-1 levels finally showed the expected 80 ng/mL increase we'd been unable to achieve with the contaminated product, and the injection site reactions that had plagued her first month disappeared entirely.
Cost considerations matter for sustainability. Most insurance won't cover off-label peptide use for fat loss, meaning you'll pay out-of-pocket for medications, consultations, and monitoring bloodwork. Monthly expenses typically range from $300-600 for peptide combinations plus $150-300 for quarterly lab work. Treatment duration of 12-16 weeks minimum means total investment of $1,500-3,500 for a single cycle.
Realistic expectations prevent disappointment and premature discontinuation. Peptides aren't magic, they're tools that might enhance fat loss by 20-40% beyond what you'd achieve through diet and exercise alone. Well, someone losing 1 pound weekly through lifestyle changes might lose 1.3-1.5 pounds weekly with peptides added. That acceleration is meaningful over 12 weeks but won't compensate for poor dietary habits or sedentary behavior.
The best candidates for peptide therapy are typically adults who've already optimized nutrition and exercise but face stubborn fat deposits or age-related metabolic slowdown. Using peptides as a first-line approach before addressing basic lifestyle factors rarely produces satisfying results and wastes considerable money on suboptimal outcomes.
Frequently Asked Questions
Is semaglutide the only FDA-approved peptide for weight loss?
Yes, semaglutide (Wegovy) is the only FDA-approved peptide specifically for weight loss in otherwise healthy adults. While tesamorelin is FDA-approved, it's only approved for lipodystrophy (abnormal fat distribution), not general obesity. Other peptides like AOD-9604 and CJC-1295 operate in a regulatory gray zone and are prescribed off-label without robust clinical trials proving efficacy in healthy weight loss.

How much weight can I realistically expect to lose with AOD-9604 or CJC-1295?
Both AOD-9604 and CJC-1295 typically produce 1.2-2.8% body fat reduction over 12 weeks in available studies. This is significantly less than semaglutide's 12.4% average weight loss. Individual results vary dramatically based on baseline hormone levels, body composition, and metabolic health, so these figures represent averages rather than guaranteed outcomes.
Why do wellness clinics prescribe peptides that aren't FDA-approved for weight loss?
These peptides target natural physiological pathways that decline with age—growth hormone production drops roughly 14% per decade after 30. Clinics argue that restoring these signals is logical, but they're prescribed off-label based on theoretical mechanisms rather than the robust clinical trials required for FDA approval. This represents a regulatory gray zone where the science is suggestive but not conclusive.
What's the difference between AOD-9604 and growth hormone-stimulating peptides like CJC-1295?
AOD-9604 is a modified growth hormone fragment that directly stimulates fat cell breakdown and blocks new fat formation without elevating overall growth hormone levels. CJC-1295 works indirectly by triggering your pituitary gland to release more GH, which then promotes fat loss. AOD-9604 may be safer for older adults concerned about cancer or diabetes risk since it avoids GH's broader effects on insulin and IGF-1 production.
How does semaglutide work differently from other fat loss peptides?
Semaglutide operates through GLP-1 receptor activation, mimicking a gut hormone that slows stomach emptying, reduces appetite signals in the brain, and enhances insulin secretion. In contrast, other peptides primarily work through growth hormone pathways to increase fat breakdown and preserve muscle. Semaglutide's appetite-suppression mechanism produces more dramatic weight loss (12.4% average) compared to other peptides.
Should older adults use different peptides than younger people for fat loss?
Yes, older adults should consider safety factors more carefully. AOD-9604 may be preferable to full growth hormone elevation since it avoids broader hormonal effects. The article specifically notes that older adults need to evaluate safety considerations, particularly regarding cancer risk and diabetes with GH-stimulating peptides. Consulting a healthcare provider about baseline hormone levels is essential before starting any peptide therapy.
What clinical evidence exists for peptides like AOD-9604 and CJC-1295?
AOD-9604 completed a 300-participant phase 2 trial in 2007 but never advanced to FDA approval, with results remaining unpublished. CJC-1295 has only small human trials and primarily observational data. This contrasts sharply with semaglutide, which has large randomized controlled trials meeting FDA standards. The evidence gap means you're working with considerably less certainty about outcomes with non-FDA-approved peptides.
Can peptides preserve muscle mass while losing fat?
Growth hormone-stimulating peptides like CJC-1295 and Ipamorelin theoretically preserve lean muscle mass during weight loss, potentially improving body recomposition rather than just reducing overall weight. However, this benefit is based on GH's known effects on muscle preservation, not on robust clinical trials specifically measuring body composition changes in weight loss patients using these peptides.